Science
Our drug candidate EL 924 designed to Address Unmet Needs in the Global Obesity and Insulin Resistance Epidemic
The Challenge
Incretine based (GLP1, GIP) weight loss drug paradox
Exceptionally effective on individual level but poorly effective to address obesity epidemic on population level
Despite the enthusiasm surrounding current and future highly effective GLP-1/GIP therapies, obesity remains a major and poorly addressed public health challenge.
Incretin-based therapies can produce substantial weight loss, but they are not the right solution for a large proportion of patients and may not be sufficient, on their own, to control the obesity epidemic at population scale.
A key limitation is poor long-term adherence, driven by reliance primarily on chronic appetite suppression, associated lean mass loss, significant GI adverse effects, and high cost. These issues limit real-world effectiveness, especially at population level.
Several state programs have already ended or restricted GLP-1 coverage for obesity and weight loss, largely due to concerns around long-term real-world effectiveness, adherence — including discontinuation even when drugs are provided at low or no cost — and budget impact.
This highlights the need for differentiated obesity therapies that patients are likely to stay on for long time – effective, well tolerated, scalable, affordable, and less dependent on chronic appetite suppression.
Elaphron’s approach is designed to address this gap
Ultimately, obesity treatment is a marathon, not a sprint. Drug efficacy alone is not enough; long-term tolerability, adherence, and patient long-term acceptability — the therapy “likability factor” — will play a major role in real-world success.
35%
100M+
Our approach and biologic basis for EL 924:
Mimicking the Profound Metabolic Benefits of Bariatric Surgery with a Simple Oral Therapy:
A Novel Approach to Obesity Beyond Appetite Suppression
Metabolic surgeries such as gastric bypass produce profound and rapid benefits in obesity, insulin resistance, diabetes, and broader metabolic health. The depth and speed of these effects exceed what has been achieved with available medical therapies.
A growing body of evidence suggests that many of these benefits are driven not simply by calorie restriction or weight loss, but by changes in food flow, intestinal nutrient sensing, bile acid signaling, and broader food-driven gut metabolic signaling. These mechanisms may help lower the metabolically defended body-weight set point. This concept is supported by human clinical observations that gastric bypass can induce diabetes remission even in non-obese patients, and by ileal transposition models, where surgical driven portion restriction (stomach size reduction) has no role.
At Elaphron, our approach is designed to mimic key aspects of this biology without surgery. EL-924 is a non-absorbed, locally acting oral therapy designed to reshape how the gut senses and responds to food, with the goal of rebalancing gut-derived metabolic signaling involved in body-weight regulation, insulin sensitivity, and broader metabolic health — similar to pathways engaged by metabolic surgery.
The Intestine as a Master Regulator of Metabolic Health and Obesity
The intestine is not only an organ of digestion and absorption. It is a powerful and highly active metabolic, immune, neural, and hormonal signaling organ that helps regulate body weight, insulin sensitivity, glucose metabolism, lipid metabolism, inflammation, feeding behavior, brain function, adipose and muscle signaling, and broader metabolic and hormonal health.
Through nutrition-driven signaling pathways
Current incretin therapies based on gut-derived hormones such as GLP-1 and GIP validate the exceptional power of intestinal hormonal signaling, but they represent only a small part of a much larger nutrition-driven gut regulatory network activated by gastric bypass.
This broader system includes Current incretin therapies based on gut-derived hormones such as GLP-1 and GIP validate the exceptional power of intestinal hormonal signaling. However, GLP-1 and GIP represent only a small part of the much broader nutrition-driven gut regulatory network engaged by gastric bypass and other metabolic surgeries.
This broader system includes multiple coordinated pathways:
Gut-derived hormonal signaling: GLP-1, GIP, PYY, ghrelin, CCK, oxyntomodulin, glicentin, neurotensin, serotonin, motilin, somatostatin, secretin, and pancreatic polypeptide.
Bile acid and metabolic signaling: bile acid circulation, FXR/TGR5 pathways, and downstream FGF19/FGF21-related signaling.
Neural signaling: vagal signaling, enteric nervous system activity, and nutrient-responsive gut-brain communication.
Nutrient sensing and epithelial biology: driven by food diversion – nutrient transporters, enteroendocrine cell activity, epithelial barrier function, intestinal ion-channel function, and local mucosal signaling.
Immune and inflammatory signaling: gut immune-cell activity, epithelial-immune interactions, and local inflammatory regulation.
Microbiome-related signaling: microbiota-derived metabolites and microbiome-mediated effects on gut and systemic metabolism.
Systemic endocrine and metabolic networks influenced by the gut: insulin, glucagon, IGF-1, adiponectin, leptin, myokines, skeletal-muscle and adipose endocrine signaling, and ceramide/ceramidase-related metabolic pathways.
Together, these pathways form a complex food-responsive regulatory network that may help explain why metabolic surgery can produce effects on weight, insulin resistance, diabetes, and cardiometabolic health that exceed what is typically achieved by targeting GLP-1/GIP signaling alone.
Modern dietary patterns may chronically disrupt this system. Highly processed, energy-dense diets can alter nutrient exposure in the proximal intestine and contribute to durable changes in intestinal epithelial cell composition, behavior, nutrient sensing, and signaling. Over time, these changes may distort how the gut responds to food, leading to dysfunctional gut-derived signaling that contributes to insulin resistance, obesity, type 2 diabetes, and broader metabolic dysfunction.
By modifying these hormonal and metabolic signals through controlled nutrient interaction, receptor modulation, ion-channel modulation, and bile acid signaling effectively mimicking gastric bypass, it may be possible to treat obesity and insulin resistance at an upstream biological control point, rather than relying solely on appetite suppression or downstream metabolic intervention.
EL 924 - Mechanism of Action, Preclinical Efficacy, Early Human Signals for Safety, Tolerability, Efficacy, Lean Mass Preservation, and Rapid Insulin-Resistance Reversal
Mechanism of Action
EL-924 is a complex, non-absorbable, locally acting, carbohydrate based metallo-heteropolymer active-compound association complex.
It is derived from a common dietary sugar that, after chemical modification, becomes non-absorbable, non-digestible, polymerizable, capable of holding functional charge, and most important able to form association complexes. Other active components are selected for favorable safety, efficacy, and poor-absorption characteristics, supporting a predominantly local intestinal effect with limited systemic exposure and potentially lower safety concerns.
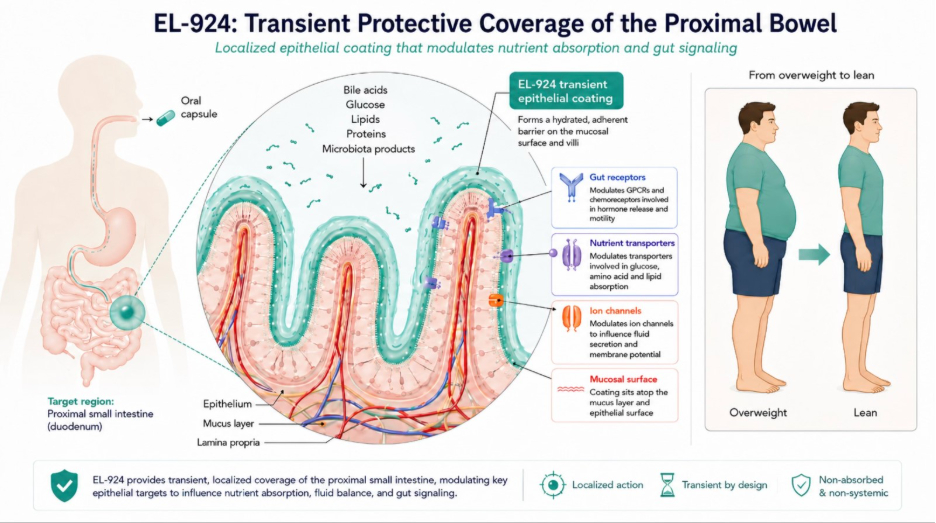
After oral intake, EL-924 creates a transient, non-absorbable protective intestinal coating that self-eliminates within hours.
Notably, many naturally occurring polymers are carbohydrate- or sugar-based, supporting the rationale for our carbohydrate-derived, non-absorbable therapeutic polymer platform.
By interacting locally with key intestinal receptors, transporters, and ion channels, EL-924 is designed to reshape how the gut responds to food and bile acid signals—potentially mimicking key food-driven, gut-mediated signaling changes observed after gastric bypass and reproducing similar metabolic benefits.
Preclinical Obesity Efficacy
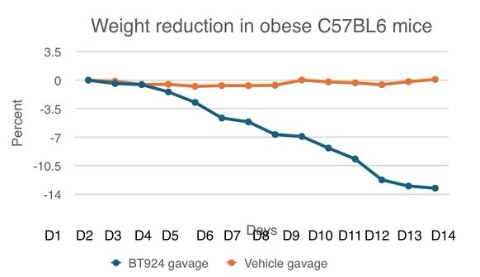
In obese mouse models (C57BL6), EL-924 produced approximately 7% weight loss per week, reaching approximately 14% weight loss by two weeks, with strong reproducibility across experiments. This magnitude is directionally comparable to historical semaglutide/Ozempic effects reported in obese mouse models.
A key differentiation factor is that EL-924’s weight-loss effect was observed without reduced food intake, altered feeding behavior, signs of feeding discomfort, diarrhea, bloating, or other observed toxicity signals. This supports a mechanism distinct from appetite suppression and suggests favorable GI tolerability in preclinical testing.
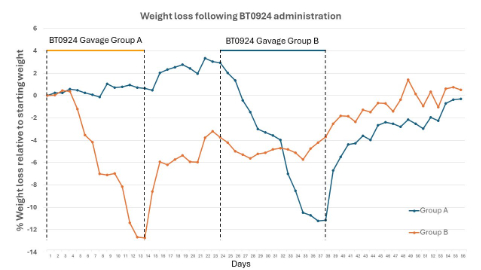
In crossover animal experiments, EL-924 demonstrated highly reproducible effects. Although partial weight regain occurred rapidly after treatment discontinuation, the weight-loss benefit persisted for approximately three times the active weight loss treatment duration. By comparison, historical GLP-1 animal data suggest return to baseline weight occurs over approximately 1.5 times the active weight loss treatment duration, supporting the possibility of a differentiated durability profile.
Early Human Observations with EL-924
Limited, non-pivotal, real-world observations N2
Limited, non-pivotal N2 real-world human observations with EL-924 (N2) have shown encouraging early signals, including exceptional tolerability, apparent safety with prolonged use, significant weight loss with preservation of lean mass, and highly favorable body-composition changes.
EL-924 was associated with approximately 30% body-fat reduction within 17 weeks, while lean mass was preserved. This is potentially differentiated from GLP-1/GIP-based therapies, where approximately 25% of total weight lost may come from lean mass, meaning larger total weight loss and longer treatment duration may be required to achieve comparable favorable body-composition changes.
EL-924 also showed a rapid and substantial insulin-resistance signal. Insulin-resistance indices improved by approximately 3-fold within 3 weeks and up to 4.8-fold within 17 weeks, moving from a prediabetic insulin-resistance range toward levels consistent with rarely seen high insulin sensitivity profile. Importantly, the initial and larger improvement occurred before significant weight loss, supporting a potential weight-loss-independent metabolic mechanism.
The magnitude and speed of this insulin-resistance signal appear directionally closer to the rapid metabolic effects observed after bariatric/metabolic surgery than to the slower, more modest, and largely weight-loss-associated insulin-sensitivity improvements typically reported with GLP-1/GIP-based therapies.
These early real-world observational signals are encouraging, but they are limited, non-pivotal, and require confirmation in controlled clinical studies.
EL-924: Key Advantages and Differentiation from Incretin-Based Therapies
Potential Role in the Obesity Treatment Ecosystem
A major differentiator for EL-924 is that preclinical weight loss was observed without reduced food intake, altered feeding behavior, signs of feeding discomfort, or significant stool changes. Early human observations also suggest strong tolerability, rapid improvement in insulin resistance before significant weight loss, and improved exercise tolerance — supporting a mechanism distinct from appetite suppression.
In preclinical models, EL-924 demonstrated weight-loss efficacy comparable to semaglutide/Ozempic.
While next-generation incretin-based therapies, including GLP-1/GIP, GLP-1/GIP/glucagon, and amylin/GLP-1 combinations, may achieve greater maximal weight loss, their effects remain largely driven by appetite suppression and altered feeding behavior, often with GI adverse effects, lean-mass loss with related delayed improved body compoition, and long-term adherence challenges.
EL-924 may therefore offer a differentiated profile for patients where Ozempic-level weight loss is sufficient, but metabolic benefit, lean-mass preservation, tolerability, and maintenance of normal eating behavior are critical.
This may be especially relevant for sarcopenic obesity, older adults, active individuals seeking to preserve strength and performance, and patients who cannot tolerate incretin-based therapies.
Mechanistically, EL-924 and incretin-based therapies may also be highly complementary, creating potential opportunities for combination use.
This creates potential for:
Sarcopenic obesity, where preservation of lean mass is clinically important
Stand-alone use in patients who cannot tolerate incretin-based therapies and when GLP1 level weight loss is enough
Stand-alone use in patients seeking weight loss without severe restriction of eating behavior, loss of food enjoyment, lean mass loss, or performance limitations
Combination therapy with GLP-1/GIP or other incretin-based agents for patients who require greater-than-GLP1-level weight loss
Lower-dose incretin combinations to improve tolerability when continuation of incretin-based therapy is desirable
Weight-loss maintenance after discontinuation of appetite-suppressive therapy, potentially allowing patients to return to more normal eating patterns with reduced risk of weight regain
Prevention or mitigation of episodic weight gain in non-obese or weight-stable individuals during periods of increased food intake, such as holidays, travel, or vacation
Potential benefits in non obese patients to control insulin resistance, in our experiments insulin resistance resolved fast before significant weight loss as well as gastric bypass surgery can effectively resolve insulin resistance and Diabetes even in non obese patients
Lean Mass Preservation
Early observations with EL-924 suggest preservation of lean mass during weight loss. Similar findings have also been reported by other group developing polymer-based nutrient-signaling therapies, suggesting this may reflect a broader method-related mechanism.
This observation is directionally supported by metabolic surgery literature. After gastric bypass, changes in gut-derived signaling have been associated with improvements in metabolic and anabolic hormone pathways, including testosterone regulation, IGF-1, and growth hormone signaling, as well as improved strength-to-weight ratio.
However, after gastric bypass, the severe calorie restriction that often occurs during the early postoperative period may still activate calorie-deficit–associated pathways that contribute to lean mass loss in extend similar to the appetite-suppression mechanism of GLP-1/GIP therapies.
In contrast, EL-924–associated weight loss was observed without reduced oral intake in preclinical studies, suggesting a potential advantage in avoiding low-calorie–driven signals that can promote lean mass preservation, while preserving anabolic benefits.
Additional supportive signals come from ileal transposition literature. This procedure alters nutrient and bile acid–driven gut signaling without relying on surgical portion restriction. In animal studies, ileal transposition has been associated with favorable body-composition changes without weight changes, with fat loss occurring alongside gain of lean mass.
The mechanistic basis for lean mass preservation remains under active investigation.
If confirmed in further clinical studies, lean mass preservation could represent an important differentiator for EL-924, particularly compared with therapies where a significant portion of total weight loss may come from lean tissue.
EL-924: Potentially Best-in-Class Nutritional Signal–Modifying Technology
Our approach—(modulating gut-derived food signaling with oral polymer-based technology to mimic key effects of metabolic surgery) —is part of a rapidly emerging field with growing scientific and commercial momentum. Currently, only a small number of startups are active in this space.
However, the category faces three major limitations that remain poorly addressed by other groups and could restrict clinical and commercial success:
Limited efficacy — other drug candidates in this space appear to show only a fraction of GLP-1/semaglutide-level weight-loss effects
GI tolerability challenges — an inherent weakness of any nutrient-diversion approaches. By forming an intestinal barrier and shifting undigested or partially digested nutrients to lower regions of the gut, these therapies may contribute to bloating, SIBO-like symptoms, nausea, diarrhea, and broader GI discomfort.
High pill burden — large amounts of material may be required to generate meaningful clinical effects
EL-924 is designed and excessively modified to address these limitations.
In preclinical studies, EL-924 demonstrated weight-loss efficacy comparable to semaglutide, with strong observed tolerability and substantially higher up to 8 folds activity per milligram of material
High efficacy per mg of material – creates the potential to reduce pill burden to a simple twice-daily oral regimen during the weight-loss phase and once-daily dosing during maintenance, while significantly improving GI tolerability and overall clinical utility.
In addition, limited, non-pivotal real-world human observations with EL-924 have shown encouraging signals, including exceptional tolerability with prolonged use, meaningful weight loss, preservation of lean mass, and rapid improvement in insulin resistance.
Limitations of Metabolic Surgery–Mimetic Approaches and Ways to Address Them
Variable response: Gut nutritional-signaling reprogramming may not work for every patient. Bariatric surgery, EndoBarrier, and epithelial resurfacing literature suggest meaningful responses in a Majority of patients (potentially 50-90%) but not for all, obesity is heterogeneous, with both non-responders and hyper-responders expected similar to GLP/GIP data.
GI tolerability: Nutrient-diversion approaches can increase delivery of undigested nutrients to lower regions of the gut, which may trigger bloating, nausea, diarrhea, and lead to SIBO. Elaphron has worked to address this through targeted modifications to EL-924’s polymer design.
Absorption monitoring: Potential effects on vitamin, micronutrient, and drug absorption are valid concerns. No meaningful vitamin or micronutrient absorption issues have been observed in our prolonged-use human observational data, but this will remain an important area for clinical monitoring.
Manageability: Bariatric surgery experience suggests nutrient or medication-absorption changes can often be managed through routine monitoring, supplementation, and medication-dose adjustment when needed similar to GLP/GIP therapies that may require supplements
Platform Extensions:
EL-615 in IBD and EL-787 in Functional GI Disorders
Insights from EL-924’s protective coating and local epithelial interaction helped inform the development of two additional gut-directed programs:
EL-615 for inflammatory bowel disease and EL-787 for functional GI disorders, including IBS-D, SIBO-like symptoms, and bloating.
EL-615:
Inflammatory Bowel Disease: Addressing Key Limitations of Current Therapies
Although the IBD treatment landscape is crowded, there remains a significant unmet need for therapies that provide rapid symptom relief without systemic immunosuppression. Current IBD therapies can take days, weeks, or even months to achieve meaningful clinical benefit, and many rely on immune suppression, which may increase risks of infection, malignancy, and other safety concerns.
EL-615 is designed as a locally acting, non-immunosuppressive therapy that forms a transient protective layer over inflamed and ulcerated intestinal tissue. By shielding damaged epithelium from harsh intraluminal conditions and disease-triggering luminal factors, EL-615 may rapidly reduce irritation, support mucosal recovery, and improve key IBD symptoms such as diarrhea and bleeding.
In validated DSS colitis models, orally administered EL-615 demonstrated rapid improvement in key disease features, including bleeding and diarrhea, with effects observed as early as 20 minutes after administration, consistent with activity beginning once the drug reaches the inflamed intestine.
In severe lethal colitis models, EL-615 showed a striking survival benefit, increasing survival from approximately 30% to 80% when administered after severe colitis was already established. This timing is important and differentiating: many immunosuppressive approaches require administration before disease establishment to show survival benefit and may have limited efficacy, or even worsen outcomes, when administered during acute severe disease.
These preclinical results suggest meaningful local activity in inflamed intestinal tissue and support EL-615’s potential as a rapid, gut-localized therapy for symptom control and potential remission induction in IBD. Its non-immunosuppressive, barrier-protective mechanism may also be highly complementary to existing immunosuppressive and biologic therapies, creating significant collaboration and combination-treatment potential rather than direct competition alone.
EL-787: Rapid Symptom Control for Bloating, SIBO-Like Symptoms, and IBS-D
Bloating is increasingly recognized as a major GI complaint in the United States, affecting a large proportion of adults and lacking highly effective treatment options.
EL-787 emerged from our work to optimize EL-924 tolerability and address potential GI effects associated with nutrient diversion, including bloating, SIBO-like symptoms, and diarrhea.
The resulting program showed encouraging potential to rapidly reduce pre-existing bloating, SIBO-like symptoms, and IBS-D–related discomfort in early human observations.
EL-787 is designed as a locally acting, potentially PRN oral therapy for common functional GI symptoms.
By providing transient protective mucosal coverage in harsh intraluminal conditions and modulating local microbiota-related interactions, EL-787 may deliver rapid and meaningful symptom relief while maintaining a favorable safety profile and promoting epithelial repair and improved defense mechanisms.
Broader Platform Validation
Together, EL-615 and EL-787 support the broader platform concept: by tuning local intestinal coating, epithelial interaction, and GI signaling, the same core technology can generate differentiated therapies across metabolic, inflammatory, functional, and secretory GI diseases.